

THE AUDIOLOGISTS AT NORTHWEST OHIO HEARING CLINIC see a wide variety of patients, from babies to adults, with issues from hearing loss and tinnitus to dizziness. Every so often, a parent will bring in their school-aged child and report that they are not hearing well. They are not doing well in school, and they have symptoms associated with hearing loss. After performing a thorough case history and audiological examination, test results show normal hearing thresholds in both ears, surprising the parent. Then they ask, what is going on? Why is my child having these issues? It is usually recommended that the child be tested for an auditory processing disorder (APD), but to many parents this term is foreign.
An APD, sometimes known as a central auditory processing disorder (CAPD), is defined by the American Speech-Hearing Association (ASHA) as an auditory deficit that is not the result of another higher-order cognitive, language, or related disorder. APD refers to how the central nervous system uses auditory information. Often APD is confused with attention deficit/hyperactivity disorder (ADHD). Though similar to APD, kids with ADHD exhibit poor listening and have difficulty remembering information, but it is not due to poor processing of auditory information in the central nervous system. Instead, it is due to their attention deficit. APD can co-exist with ADHD.
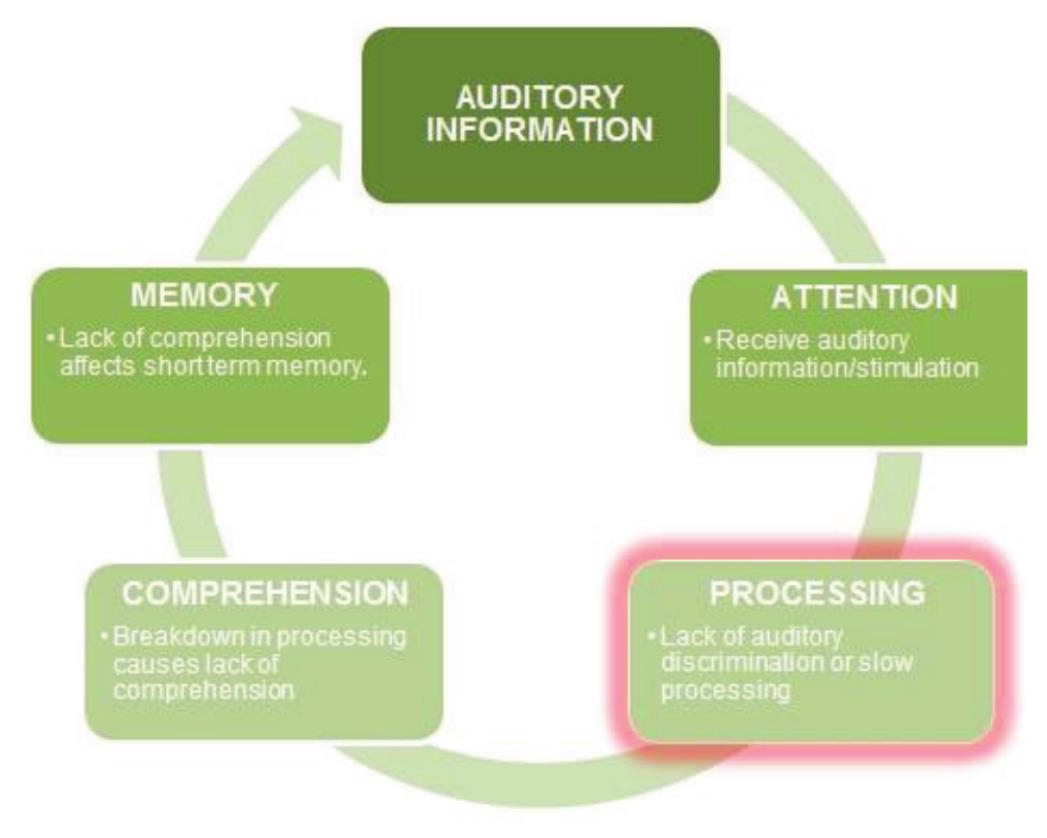
The graphic below describes what happens in a child or adult with APD.
(Auditory Processing Disorder Foundation, Inc.)
APD symptoms can range from very mild to severe. Some common behaviors associated with APD include (but are not limited to):
• Difficulty understanding in noisy environments
• Difficulty following multi-task directions
• Difficulty discriminating between similar speech sounds
• Often asking for repetition or clarification
• Difficulty with spelling, reading, and understanding direction in school
• Difficulty understanding jokes or riddles
• Performs better in quiet environments
• Does better in classes that don’t involve heavy listening.
Though, there is no known cause of APD, According the ASHA, a multidisciplinary team approach is critical to fully assess and understand the cluster of problems exhibited by children with APD. This team includes the child’s teacher to describe any academic issues, a psychologist to evaluate cognitive function, and a speech-language pathologist to investigate written and oral language, speech, and related capabilities. Yet it is important to know that, however valuable the information from the multidisciplinary team is in understanding the child’s overall areas of strength and weakness, none of the test tools used by these professionals are diagnostic tools for APD and the actual diagnosis of APD must be made by an audiologist.
Evaluation for APD involves a series of tests done through headphones. An audiological evaluation is performed first to rule out any type of hearing loss. The APD tests are usually performed in a sound-proof booth and involve listening to a variety of words or sentences in background noise or separated into each ear where the listener must repeat what is being said inear only. Most APD tests require a child to be at least seven years of age. The test results will show if there is a deficit and what type. Once this is determined, the appropriate treatment can be determined.
Once APD has been diagnosed, treatment can then begin. It is important to know that treatment for APD is very individualized and deficit-specific. What may have worked for one person may not work for the next. Treatment of APD generally focuses on three primary areas. The first two are changing the learning or communication environment by improving access to auditorily presented information, and recruiting higher-order strategies to help compensate for the disorder. These strategies usually consist of suggestions for assisting listeners in strengthening central resources (language, problem-solving, memory, attention, and other cognitive skills) so that they can be used to help overcome the auditory disorder. The last treatment area is remediation of the auditory deficit itself by using computer-based training or training with a therapist (ASHA). Improvement of the deficit cannot be determined in advance. Some children seem to grow out of their deficit while others may have a small degree of the deficit forever.
At home, making a few accommodations will make like easier for your child: always talk facing your child when possible, decreasing any background noise; make instructions simple and have them repeat them back to you; make sure homework is done in a quiet place; speak at a slightly slower rate so your child can process what is being said; and, finally, be patient. Kids have such a hard time on a daily basis trying to sort everything out in their brains, and a little patience goes a long way.
If you believe you or your child may have an APD, the first step is to have your hearing tested. At Northwest Ohio Hearing Clinic, we can do this for you. If the test results and/or case history indicate APD, we can make the appropriate referral for you to get testing and/or treatment. Please call one of our offices to schedule an appointment.
Dianna Randolph, AuD, CCC-A, is a Doctor of Audiology with Northwest Ohio Hearing Clinic, located at 1125 Hospital Dr., Suite 50 in Toledo (419-383-4012) and 1601 Brigham Dr., Suite 160 in Perrysburg (419-873-4327).
